1. Fundamental Radiation Protection Principles
According to the International Atomic Energy Agency (IAEA), protection against internal exposure follows the same three fundamental principles applied to all radiation exposure situations.
- Justification
Any practice that may result in internal exposure, such as handling radioactive materials or nuclear medicine procedures, must produce a net benefit. In other words, no activity involving the potential intake of radionuclides should be undertaken unless it is clearly justified. - (2) Optimization (ALARA Principle)
Radiation exposure must be kept as low as reasonably achievable (ALARA), taking into account economic and societal factors. For internal exposure, this principle emphasizes minimizing radionuclide intake, controlling contamination pathways, and reducing the resulting committed dose through appropriate design and operational practices. - (3) Dose Limitation
Individual radiation doses must remain within regulatory limits. For occupational exposure, this is typically 20 mSv per year averaged over five years, while for the general public it is 1 mSv per year. In the case of internal contamination, these limits apply to the committed effective dose, which accounts for radiation delivered over time following intake.
2. Specific Principles for Internal Contamination Control
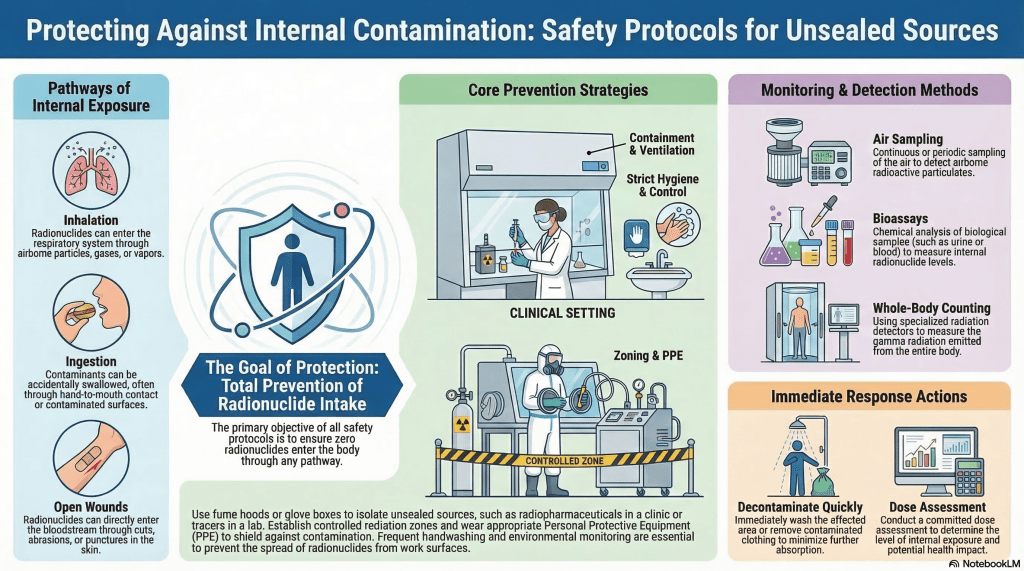
(2.1) Prevention of Intake (Primary Objective)
The central objective of internal radiation protection is to prevent radionuclides from entering the body. Intake may occur through inhalation of airborne particles, ingestion of contaminated materials, or absorption through wounds or damaged skin.
Effective prevention relies on engineering controls such as containment systems (e.g., glove boxes and hot cells), ventilation with HEPA filtration, and controlled work zones. Personal protective equipment, including respirators, gloves, and protective clothing, provides additional protection when necessary.
(2.2) Control of the Working Environment
The working environment must be carefully controlled to limit the spread of contamination. This includes the use of zoning systems to distinguish controlled and supervised areas, adherence to surface contamination limits, and regulation of airborne radioactivity through Derived Air Concentration (DAC) values.
Engineering measures such as fume hoods, local exhaust ventilation, and negative pressure systems are essential to ensure that radioactive materials remain confined and do not disperse into the workplace.
(2.3) Monitoring and Detection (Instrumentation Requirements)
Since internal exposure cannot be directly measured by external dosimeters, indirect monitoring using specialized instruments is essential.
Workplace monitoring typically involves air sampling systems, continuous air monitors (CAMs), and surface contamination survey meters (e.g., Geiger–Müller or scintillation detectors). These instruments provide early detection of airborne and surface contamination.
Individual monitoring is performed using bioassay techniques (such as urine and fecal analysis) and in vivo measurement systems, including whole-body counters and thyroid monitors. These tools are critical for assessing radionuclide intake and estimating internal dose.
(2.4) Dose Assessment (Committed Dose Concept)
Internal exposure is evaluated using the concept of committed dose, which reflects radiation delivered over time after intake. The key quantities include the committed effective dose (E₅₀) and the committed equivalent dose (H₅₀).
These values depend on the radionuclide involved, its physical and chemical form, and its behavior within the body, as described by biokinetic models developed by the ICRP. Such models account for the distribution, retention, and clearance of radionuclides in different organs.
(2.5) Contamination Control and Decontamination
If contamination occurs, prompt action is required to minimize further intake and prevent spread. This includes the immediate removal of contaminated clothing, gentle washing of affected skin, and isolation of the contaminated area.
In the workplace, decontamination involves surface cleaning, waste segregation, and verification using contamination monitoring instruments to ensure that levels have been reduced to acceptable limits.
(2.6) Medical Management of Internal Contamination
In cases of significant intake, medical intervention may be necessary. The IAEA recommends the use of decorporation therapies, which reduce radionuclide absorption and enhance elimination from the body.
Examples include the administration of stable iodine (KI) for radioactive iodine, Prussian blue for cesium-137, and DTPA for actinides. The effectiveness of these treatments depends strongly on early application following exposure.
(2.7) Training and Safety Culture
A strong safety culture is essential for effective protection. Workers must be trained to understand contamination risks, follow proper handling procedures, use monitoring instruments correctly, and respond appropriately to incidents. Regular training and drills ensure preparedness and consistent application of safety measures.
3. Key Quantities and Concepts
Several key quantities are used in internal radiation protection. Intake refers to the amount of radionuclide entering the body. The Annual Limit on Intake (ALI) defines the maximum permissible intake corresponding to dose limits, while the Derived Air Concentration (DAC) represents the airborne activity level that would lead to the ALI under defined conditions. The committed dose describes the total radiation dose delivered over time following intake, and biokinetic models are used to describe the distribution and retention of radionuclides within the body.
4. Hierarchy of Controls (IAEA Approach)
The IAEA emphasizes a layered approach to protection. The highest priority is given to elimination or substitution of radioactive materials where possible. This is followed by engineering controls such as containment and ventilation, then administrative controls including procedures and zoning. Personal protective equipment represents the final layer of defense and should not be relied upon as the primary protective measure.
5. Emergency Considerations
In situations involving accidental intake, rapid response is essential. This includes immediate assessment of intake, early administration of blocking or decorporation agents when appropriate, and implementation of monitoring and dose reconstruction. Long-term medical follow-up may be required to evaluate potential health effects and ensure proper clinical management.
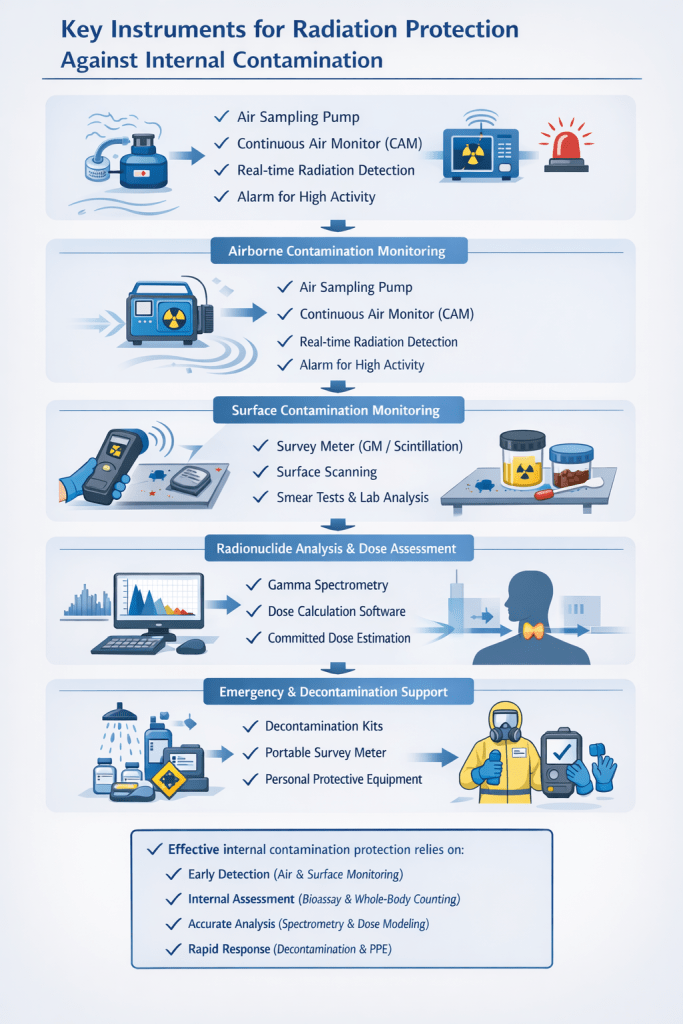
6. Key Instruments for Radiation Protection Against Internal Contamination
Effective control of internal contamination relies not only on principles and procedures but also on the availability and proper use of specialized radiation detection and monitoring instruments. These instruments support prevention, early detection, dose assessment, and response.
6.1. Airborne Contamination Monitoring
Because inhalation is the most critical intake pathway, monitoring airborne radioactivity is essential.
- Air Sampling Pumps (with filter media)
Used for periodic collection of airborne particulates, followed by laboratory analysis (e.g., alpha/beta counting, gamma spectrometry). - Continuous Air Monitors (CAMs)
Provide real-time detection of airborne activity and trigger alarms when preset levels are exceeded.
→ Critical for high-risk areas such as hot cells and radiochemical laboratories.
6.2. Surface Contamination Monitoring
To prevent ingestion and secondary spread, surface contamination must be routinely checked.
- Portable Contamination Survey Meters
Typically based on Geiger–Müller (GM) or scintillation detectors
→ Used for:- Work surfaces
- Equipment
- Personnel (hands, clothing)
- Smear (Swipe) Test + Counting Systems
Indirect method to quantify removable contamination using laboratory counters.
6.3. Personal Monitoring for Internal Exposure
Since internal dose cannot be measured externally, bioassay and in vivo systems are essential.
- Bioassay Analysis Systems
Laboratory-based measurement of radionuclides in:- Urine
- Feces
→ Used to estimate intake and committed dose
- Whole-Body Counters (WBC)
Detect gamma-emitting radionuclides within the body
→ Key tool for internal dose assessment - Thyroid Monitors
Specialized detectors for radionuclides such as iodine-131
→ Important in nuclear medicine and reactor-related incidents
6.4. Dose Assessment and Analytical Tools
To interpret measurement data, additional tools are required:
- Gamma Spectrometry Systems (HPGe detectors)
High-resolution identification and quantification of radionuclides in samples - Dose Assessment Software (ICRP-based models)
Used to calculate:- Committed effective dose (E₅₀)
- Organ doses
Based on intake data and biokinetic models
6.5. Decontamination and Emergency Support Equipment
In contamination events, rapid response requires dedicated tools:
- Portable Decontamination Kits
Including washing solutions, absorbent materials, and protective supplies - Portable Survey Meters for Clearance Checks
Used to confirm successful decontamination - Personal Protective Equipment (PPE)
Although not a detector, PPE (respirators, gloves, protective suits) is essential to prevent further intake during response
6.6. Integrated Monitoring Systems
In advanced facilities, instruments are often integrated into a radiation protection monitoring system, including:
- Fixed area monitors
- Alarm systems
- Data logging and centralized control
→ These systems provide continuous oversight and enhance safety management.
Summary
The most critical instruments for internal contamination protection include:
- Continuous Air Monitors (CAMs) → early warning of inhalation risk
- Contamination Survey Meters → control of surfaces and personnel
- Bioassay and Whole-Body Counters → assessment of internal dose
- Gamma Spectrometry Systems → radionuclide identification
- Dose Calculation Tools → interpretation and regulatory compliance
Together, these instruments form the core technological backbone of internal radiation protection, enabling both prevention and accurate dose assessment in accordance with IAEA recommendations.
Table: Radiation Protection Instruments for Internal Contamination Monitoring
| Instrument | Primary Function | Radiation Type Detected | Typical Sensitivity / Characteristics |
| Air Sampling Pump (Filter-based) | Collect airborne radioactive particles for subsequent laboratory analysis | α, β, γ (depends on analysis method) | High sensitivity after counting; detection limits ~Bq/m³ (integrated sampling); not real-time |
| Continuous Air Monitor (CAM) | Real-time monitoring of airborne radioactivity with alarm capability | α, β (most common), sometimes γ | High sensitivity for airborne contamination; real-time detection (~Bq/m³); rapid response |
| Portable GM Survey Meter | Surface contamination detection and general area monitoring | β, γ (limited α with special probe) | Moderate sensitivity; fast response; limited energy discrimination; robust and widely used |
| Scintillation Survey Meter (ZnS, NaI(Tl)) | High-sensitivity contamination survey (especially low-level contamination) | α (ZnS), β/γ (NaI(Tl)) | Higher sensitivity than GM; good for low-level detection; faster response; moderate energy resolution |
| Smear (Swipe) Test + Counter (e.g., proportional counter, liquid scintillation) | Quantitative measurement of removable surface contamination | α, β (primarily) | Very high sensitivity (down to Bq level); laboratory-based; not real-time |
| Whole-Body Counter (WBC) | In vivo measurement of radionuclides inside the human body | γ (primarily) | High sensitivity (~tens of Bq depending on radionuclide); good for internal dose assessment; requires shielding |
| Thyroid Monitor | Measurement of radioiodine uptake in the thyroid gland | γ (low-energy photons, e.g., I-131) | Very high sensitivity for iodine (~Bq level); rapid screening capability |
| Bioassay (Urine/Fecal Analysis) | Indirect assessment of radionuclide intake and excretion | α, β, γ (depends on analysis technique) | Very high sensitivity; detects long-term intake; requires laboratory analysis and modeling |
| Gamma Spectrometry (HPGe Detector) | Identification and quantification of radionuclides in samples | γ (high resolution) | Excellent energy resolution; very high sensitivity (Bq or lower); laboratory-based |
| Liquid Scintillation Counter (LSC) | Measurement of low-energy beta emitters (e.g., tritium, C-14) | β (low energy) | Extremely high sensitivity for low-energy β; detection limits down to very low Bq |
| Portable Dose Assessment Software (ICRP-based models) | Calculation of committed effective dose (E₅₀) from intake data | Not a detector (analytical tool) | High accuracy depending on input data; essential for regulatory compliance |
| Portable Contamination Monitor (Frisker) | Rapid screening of personnel contamination (hands, clothing) | α, β (primarily), some γ | High sensitivity for surface contamination; fast response; field use |
Key References
- IAEA GSR Part 3 – Radiation Protection and Safety of Radiation Sources
- IAEA GSG-7 – Occupational Radiation Protection
- IAEA Safety Reports Series No. 37 – Assessment of Occupational Exposure due to Intakes
- IAEA EPR-Internal Contamination Guidelines
- หลักการป้องกันอันตรายจากการปนเปื้อนกัมมันตรังสีเข้าสู่ภายในร่างกาย
1. หลักการพื้นฐานของการป้องกันอันตรายจากรังสี
ตามแนวทางของ International Atomic Energy Agency การป้องกันการได้รับรังสีภายในร่างกายยึดตามหลักการพื้นฐาน 3 ประการเช่นเดียวกับการได้รับรังสีทุกกรณี ได้แก่ ความสมเหตุสมผล การทำให้เกิดการรับรังสีน้อยที่สุดเท่าที่สมเหตุสมผล และการจำกัดปริมาณรังสี
(1) การประเมินความคุ้มค่า (Justification)
การดำเนินกิจกรรมใด ๆ ที่อาจก่อให้เกิดการรับรังสีภายใน เช่น การจัดการสารกัมมันตรังสีหรือการใช้ในทางการแพทย์ ต้องก่อให้เกิดประโยชน์สุทธิอย่างชัดเจน กล่าวคือ ไม่ควรดำเนินกิจกรรมใดที่มีความเสี่ยงต่อการรับสารกัมมันตรังสีเข้าสู่ร่างกายโดยไม่มีเหตุผลที่เหมาะสม
(2) การทำให้เกิดการรับรังสีน้อยที่สุดเท่าที่สมเหตุสมผล (ALARA)
การได้รับรังสีต้องถูกควบคุมให้อยู่ในระดับต่ำที่สุดเท่าที่สามารถทำได้ โดยคำนึงถึงปัจจัยด้านเศรษฐกิจและสังคม สำหรับกรณีการปนเปื้อนเข้าสู่ภายใน จะเน้นที่การลดการรับสารกัมมันตรังสีเข้าสู่ร่างกาย การควบคุมเส้นทางการปนเปื้อน และการลดปริมาณรังสีสะสมที่เกิดขึ้นในระยะยาว
(3) การจำกัดปริมาณรังสี (Dose Limitation)
ปริมาณรังสีที่บุคคลได้รับต้องไม่เกินค่าที่กำหนดตามข้อบังคับ โดยทั่วไป ผู้ปฏิบัติงานมีขีดจำกัดเฉลี่ย 20 มิลลิซีเวิร์ตต่อปี (เฉลี่ย 5 ปี) และประชาชนทั่วไป 1 มิลลิซีเวิร์ตต่อปี สำหรับการได้รับรังสีภายใน จะพิจารณาจากปริมาณรังสีสะสมระยะยาว (committed effective dose) หลังจากมีการรับเข้าสู่ร่างกาย
2. หลักการเฉพาะสำหรับการควบคุมการปนเปื้อนเข้าสู่ภายใน
2.1 การป้องกันการรับเข้าสู่ร่างกาย (เป้าหมายหลัก)
หัวใจสำคัญของการป้องกันคือการไม่ให้สารกัมมันตรังสีเข้าสู่ร่างกาย ซึ่งสามารถเกิดขึ้นได้ผ่านการหายใจ การรับประทาน หรือการซึมผ่านบาดแผล
มาตรการสำคัญ ได้แก่ ระบบกักเก็บสาร การระบายอากาศร่วมกับแผ่นกรองประสิทธิภาพสูง (HEPA) การกำหนดเขตควบคุม และการใช้อุปกรณ์ป้องกันส่วนบุคคล เช่น หน้ากากป้องกัน ถุงมือ และชุดป้องกัน
2.2 การควบคุมสภาพแวดล้อมการทำงาน
สภาพแวดล้อมต้องได้รับการควบคุมอย่างเข้มงวดเพื่อลดการแพร่กระจายของการปนเปื้อน โดยใช้การแบ่งเขตพื้นที่ การกำหนดค่าการปนเปื้อนพื้นผิว และการควบคุมความเข้มข้นของสารกัมมันตรังสีในอากาศ (Derived Air Concentration: DAC)
ระบบดูดไอ การระบายอากาศเฉพาะจุด และระบบความดันลบ มีบทบาทสำคัญในการป้องกันการฟุ้งกระจายของสารกัมมันตรังสี
2.3 การตรวจวัดและเฝ้าระวัง (เครื่องมือที่จำเป็น)
เนื่องจากการได้รับรังสีภายในไม่สามารถวัดได้โดยตรง จำเป็นต้องใช้เครื่องมือเฉพาะทางในการตรวจวัดทางอ้อม
- การตรวจวัดในพื้นที่ทำงาน ใช้เครื่องเก็บตัวอย่างอากาศ เครื่องตรวจวัดอากาศแบบต่อเนื่อง (CAM) และเครื่องสำรวจการปนเปื้อนพื้นผิว เช่น หัววัดแบบไกเกอร์-มึลเลอร์ (Geiger–Müller) หรือแบบเรืองแสงวาบ
- สำหรับบุคคล ใช้วิธีวิเคราะห์ตัวอย่างชีวภาพ (bioassay) เช่น ปัสสาวะและอุจจาระ รวมถึงการตรวจวัดในร่างกาย เช่น เครื่องนับรังสีทั้งร่างกาย และเครื่องตรวจต่อมไทรอยด์ ซึ่งมีความสำคัญต่อการประเมินปริมาณรังสีภายใน
2.4 การประเมินปริมาณรังสี (แนวคิดปริมาณรังสีสะสม)
การประเมินใช้ค่าปริมาณรังสีสะสมระยะยาว ได้แก่
- ปริมาณรังสีสมมูลสะสม (H₅₀)
- ปริมาณรังสีมีผลสะสม (E₅₀)
ค่าดังกล่าวขึ้นอยู่กับชนิดของสารกัมมันตรังสี รูปแบบทางกายภาพและเคมี และพฤติกรรมในร่างกาย ซึ่งอธิบายด้วยแบบจำลองชีวพลศาสตร์ (biokinetic models)
2.5 การควบคุมและกำจัดการปนเปื้อน
เมื่อเกิดการปนเปื้อน ต้องดำเนินการทันที เช่น การถอดเสื้อผ้าที่ปนเปื้อน การล้างผิวหนังอย่างระมัดระวัง และการจำกัดการแพร่กระจาย
ในระดับพื้นที่ ต้องมีการทำความสะอาดพื้นผิว การแยกของเสีย และตรวจสอบซ้ำด้วยเครื่องมือวัดเพื่อยืนยันความปลอดภัย
2.6 การดูแลทางการแพทย์
กรณีมีการรับเข้าสู่ร่างกายในระดับสูง อาจต้องใช้การรักษาเพื่อลดการสะสมของสาร เช่น
- ไอโอดีนเสถียร (KI) สำหรับไอโอดีนกัมมันตรังสี
- ปรัสเซียนบลู สำหรับซีเซียม-137
- ดีทีพีเอ (DTPA) สำหรับธาตุกลุ่มแอกทิไนด์
ประสิทธิภาพขึ้นอยู่กับการให้การรักษาอย่างรวดเร็ว
2.7 การฝึกอบรมและวัฒนธรรมความปลอดภัย
การสร้างความตระหนักและวัฒนธรรมความปลอดภัยเป็นสิ่งสำคัญ ผู้ปฏิบัติงานต้องเข้าใจความเสี่ยง ปฏิบัติตามขั้นตอนอย่างถูกต้อง และใช้เครื่องมือวัดได้อย่างเหมาะสม
3. ปริมาณและแนวคิดสำคัญ
ตัวแปรสำคัญ ได้แก่ ปริมาณการรับเข้าสู่ร่างกาย (intake) ขีดจำกัดการรับเข้าสู่ร่างกายต่อปี (ALI) และความเข้มข้นในอากาศที่ยอมรับได้ (DAC) รวมถึงปริมาณรังสีสะสมและแบบจำลองชีวพลศาสตร์ที่ใช้ในการอธิบายพฤติกรรมของสารในร่างกาย
4. ลำดับชั้นของมาตรการควบคุม
แนวทางของ IAEA ให้ความสำคัญกับการควบคุมแบบเป็นลำดับ ได้แก่
การหลีกเลี่ยงหรือทดแทน → การควบคุมทางวิศวกรรม → การควบคุมเชิงบริหาร → อุปกรณ์ป้องกันส่วนบุคคล
โดยอุปกรณ์ป้องกันส่วนบุคคลเป็นเพียงด่านสุดท้าย
5. การตอบสนองในกรณีฉุกเฉิน
เมื่อเกิดการรับสารเข้าสู่ร่างกายโดยไม่ตั้งใจ ต้องดำเนินการอย่างรวดเร็ว ได้แก่ การประเมินการรับเข้า การให้สารยับยั้งหรือขับออก การตรวจวัด และการติดตามผลทางการแพทย์ระยะยาว
6. เครื่องมือสำคัญสำหรับการป้องกันการปนเปื้อนเข้าสู่ภายใน
การป้องกันที่มีประสิทธิภาพจำเป็นต้องอาศัยเครื่องมือเฉพาะทางเพื่อการตรวจพบล่วงหน้า การประเมิน และการตอบสนอง
6.1 การตรวจวัดในอากาศ
ใช้เครื่องเก็บตัวอย่างอากาศและเครื่องตรวจวัดอากาศแบบต่อเนื่อง (CAM) เพื่อเฝ้าระวังการฟุ้งกระจาย โดยเฉพาะในพื้นที่เสี่ยงสูง
6.2 การตรวจวัดการปนเปื้อนพื้นผิว
ใช้เครื่องสำรวจแบบพกพา และการทดสอบแบบป้ายเช็ด (smear test) เพื่อตรวจสอบการปนเปื้อนที่สามารถแพร่กระจายได้
6.3 การตรวจวัดในร่างกาย
ใช้การวิเคราะห์ชีวภาพ เครื่องนับรังสีทั้งร่างกาย และเครื่องตรวจต่อมไทรอยด์ เพื่อประเมินปริมาณรังสีภายใน
6.4 การวิเคราะห์และคำนวณปริมาณรังสี
ใช้เครื่องวิเคราะห์รังสีแกมมา (HPGe) และโปรแกรมคำนวณตามแบบจำลองของ ICRP เพื่อประเมินปริมาณรังสีสะสม
6.5 อุปกรณ์สนับสนุนการกำจัดการปนเปื้อน
ประกอบด้วยชุดทำความสะอาด เครื่องตรวจวัดแบบพกพา และอุปกรณ์ป้องกันส่วนบุคคล
6.6 ระบบเฝ้าระวังแบบบูรณาการ
รวมเครื่องตรวจวัดประจำที่ ระบบเตือนภัย และระบบบันทึกข้อมูล เพื่อเพิ่มประสิทธิภาพในการควบคุมความปลอดภัย
สรุป
การป้องกันการปนเปื้อนเข้าสู่ภายในที่มีประสิทธิภาพต้องอาศัย
✔ การตรวจพบตั้งแต่ระยะแรก
✔ การประเมินภายในร่างกายอย่างถูกต้อง
✔ การวิเคราะห์ที่แม่นยำ
✔ การตอบสนองอย่างรวดเร็ว
โดยมีเครื่องมือวัดและระบบเฝ้าระวังเป็นแกนหลักในการดำเนินงานให้สอดคล้องกับแนวทางของ IAEA

ใส่ความเห็น